Tracking humanitarian surge response: from the Nepal earthquake to the Rohingya crisis
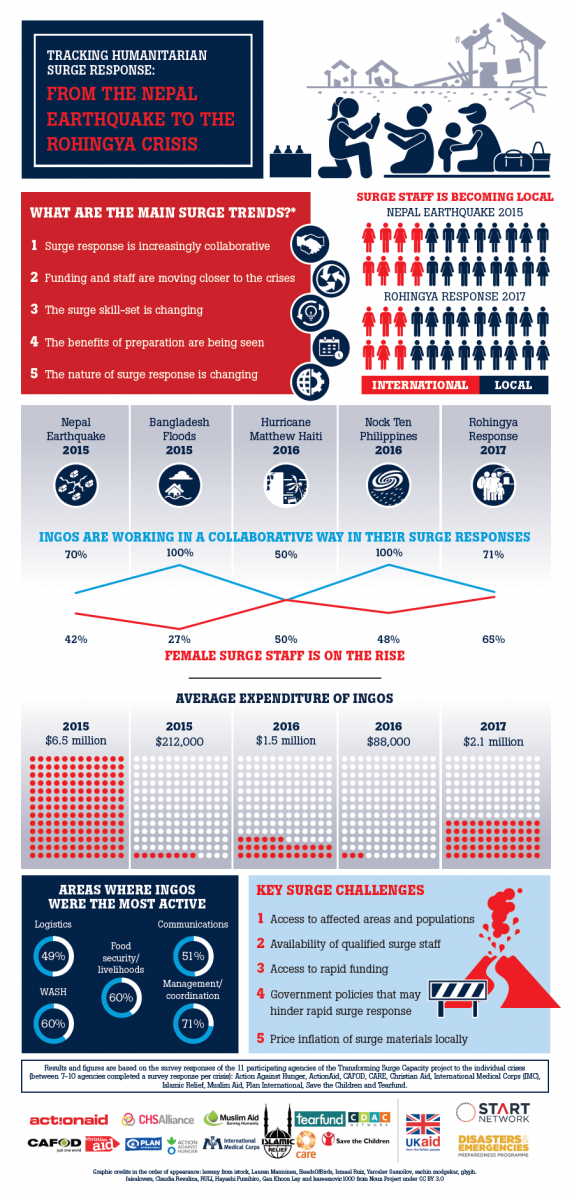
Over three years, as part of the Transforming Surge Capacity Project, which came to an end in December 2017, the research team tracked six crises to see how surge practices were changing. In this blog, I highlight five main trends from the research:
1. Surge response is increasingly collaborative but… Our research showed that all international NGOs we tracked* worked in a collaborative way in their surge responses to crises such as the Bangladesh floods of 2016 and the Philippines Nock Ten Typhoon of 2016. However, we observed that INGOs reporting on collaboration dropped in certain cases. For example, with regard to Hurricane Matthew in Haiti 50% and to the Rohingya response of 2017 71% of the INGOs reported on collaboration. Why? We found that the drop in collaborative surge was often due to context. The responses in the Philippines and Bangladesh were largely locally led where organisations and their staff had ongoing relationships and partnerships that facilitated collaboration. In Haiti, not all INGOs had established relations with local organisations citing the difficulties to do so. For the Rohingya response, the restrictions placed by the authorities meant that some INGOs were limited in their presence on the ground and needed to work remotely through other actors changing the nature of collaboration.
2. Funding and staff are moving closer to the crises as local capacity and knowledge are valued more. Over the past three years, we saw new funding opportunities open up for INGOs and their local partners, such as the Start Fund that funded responses to the Bangladesh floods and Nock Ten. Increasingly, INGOs reported sourcing surge staff locally or from the region with a 1:3 ratio seen for international to local staff for the Rohingya crisis (compared to a 1:2 ratio for the Nepal earthquake response). At the same time, the two most constant challenges seen were rapid access to funding (particularly for local partners) and finding qualified staff.
3. The surge skill-set is changing. While coordination, food security and WASH were the areas where the INGOs were most active across crises, new roles and areas (or “old” roles/areas with renewed emphasis) emerged. We saw increases in the need for cash programming, gender, protection and communications, in addition to the ability to work with local partners and to understand the humanitarian-development nexus.
4. The benefits of preparation are being seen. INGOs and partners had placed emphasis on preparation and planning in the past three years, such as: establishing partnerships and relationships with local actors and other stakeholders, investing in staff training, defining roles of existing staff for crises, putting in place surge plans and systems and pre-arranging access to funding for crises. Examples were seen where such preparation brought benefits such as quicker, more appropriate and sustainable responses.
5. The nature of surge response is changing. Over the past three years, the very nature of surge response has changed. In all contexts reviewed, the capacity of local actors and authorities has increased, challenging the surge coordination and leadership traditionally led by UN and INGOs. Humanitarian organisations are moving towards women-led responses, greater community participation and collaboration in key areas such as training, rosters, and needs assessments. The role of the typical expatriate roving surge responder is not yet extinct but they now tend to be more “home grown” and from the region (at least for Asia where the surge tracking focused on).
The six tracking reports are available online and global learnings from the project are found in the Future of Humanitarian Surge report.
*The 11 operational agencies of the project were: Action Against Hunger, ActionAid, CAFOD, CARE, Christian Aid, International Medical Corps (IMC), Islamic Relief, Muslim Aid, Plan International, Save the Children and Tearfund. Non-operational agencies were the CDAC Network and the CHS Alliance.